OSCE Pre final examination
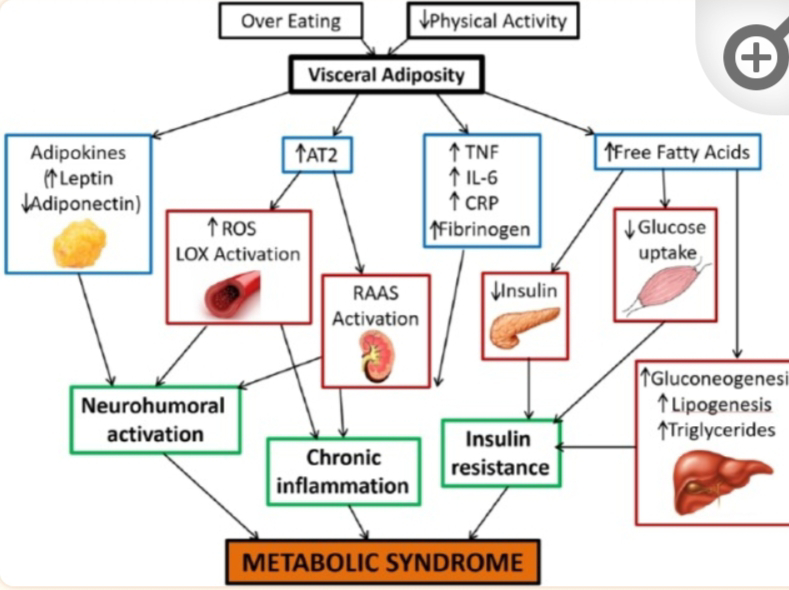
What is the pathway of metabolic syndrome Metabolic Syndrome Metabolic Syndrome represent a cluster of metabolic abnormalities that include hypertension,central obesity , insulin resistance and dyslipidemia and is strongly associated with increased risk of developing diabetes and atherosclerotic and non atherosclerotic cardiovascular disease . The pathogenesis of metabolic Syndrome involves both genetic and acquired factors that contribute to the final pathway of inflammation. Difference between seizure and pseudo seizure 1) During an attack findings such as asynchronous or side to side movement, crying, eye closure suggest pseudo seizure whereas occurance during night suggest true seizure. 2) lack of any symptoms and memory of the attack suggest pseudo seizure whereas confusion , stertorous breathing suggest true seizure. Learning points 1)Importance of proper history taking and prior treatment taken . 2)Importance of early diagnosis and ...